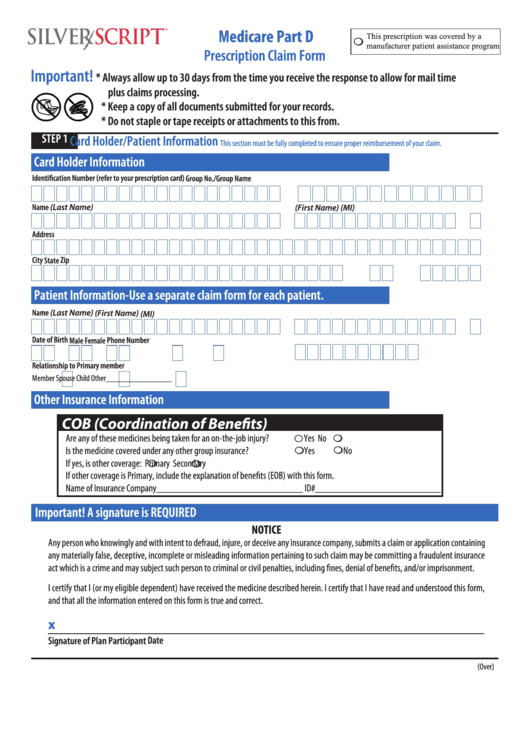
Medicare Part D Claim Form
Medicare Part D Claim Form - Instructions for completing this form. This form can be used to request reimbursement for any of the following medicare part d prescription drug benefits: If you have original medicare , the law requires your doctor, provider, or supplier to file medicare claims for covered services and supplies you get. This form can be used to request reimbursement for any of the following medicare part d prescription drug situations:
Medicare Two Way Claim 20202024 Form Fill Out And Sign Printable Pdf Template Airslate Signnow
This form can be used to request reimbursement for any of the following medicare part d prescription drug benefits: If completing this form on behalf of a medicare part d member, a valid cms 1696 appointment of representative form (or equivalent) is required visit www.cms.gov for a.
Complete One Form Per Member.
Learn about the types of costs you’ll pay in a medicare drug plan. This form can be used to request reimbursement for any of the following medicare part d prescription drug benefits: Medicare part d claim form.
Complete One Form Per Member.
By checking this box, you consent to our data privacy policy. Use this form to request reimbursement for covered medications purchased at retail cost. Your complete claim will be processed within 14 days of receipt of your request.
Always Use Pharmacies Within.
2016 part d payment rules say that your doctor must: Get forms to file a claim, set up recurring premium payments, and more. The submission of this claim form authorizes the release of all information to applicable healthcare providers and all others involved in filling the prescriptions or processing the.
Please Allow Additional Mail Time.
Use this form to request reimbursement for covered medications purchased at retail cost. It is a fillable online form. Costs for medicare drug coverage.
Medicare Part D Claim Form.
Please allow additional mail time. This form is used to submit a claim for medical payment to medicare for services or supplies that are not covered by medicare part d. Part d (medicare drug coverage) helps cover cost of.
Get All Forms In Alternate Formats.

Fill Free fillable Form 1 MEDICARE PART D CLAIM FORM (United Healthcare) PDF form

When Can You Claim Medicare

Oral Cancer Treatment Claim Processing Guide
Fillable Medicare Part D Prescription Claim Form printable pdf download

Medicare 1500 Claim Form Form Resume Examples 3q9Jk633YA

(PDF) Assessing Medicare Part D Claim Completeness Using Medication SelfReports The Role of

Application For Medicare Part B Employer Form Employment Form

Medicare part d form Fill out & sign online DocHub

Medicare Claim Form Cms 1490s Form Resume Examples djVaBnG2Jk

Medicare Standard Form 5510 Instructions Form Resume Examples Kw9kb0K2JN

Medicare Claim Form Cms 1490s Form Resume Examples djVaBnG2Jk

20132024 Aetna Vision Services Claim Form Fill Online, Printable, Fillable

How To Apply For Medicare A And B

Fill Free fillable Form 1 MEDICARE PART D CLAIM FORM (United Healthcare) PDF form

Fillable Online MedicarePartDClaimForm Fax Email Print pdfFiller
